Surgical techniques for Pectus Excavatum
Surgical correction must be planned suitably – it includes a well-informed consent and a complete preoperative analysis. It is recommendable to be familiar with this kind of surgery and to know all the potential complications and the way to solve them.
Basically there exist two procedures for the surgical correction:
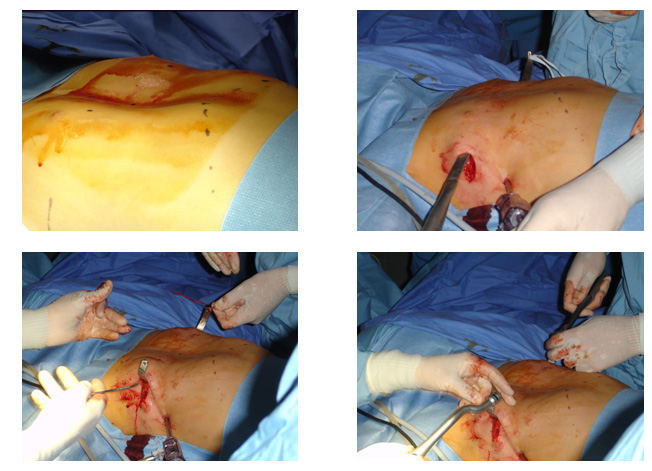
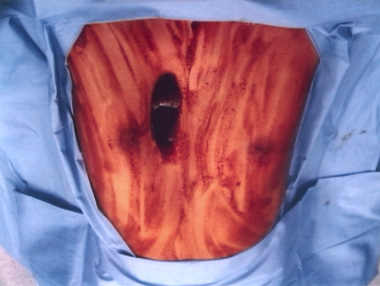
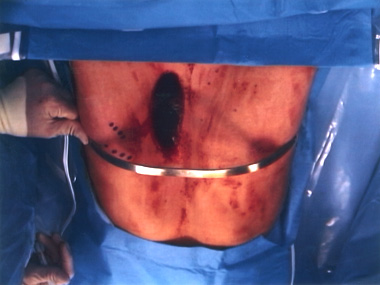
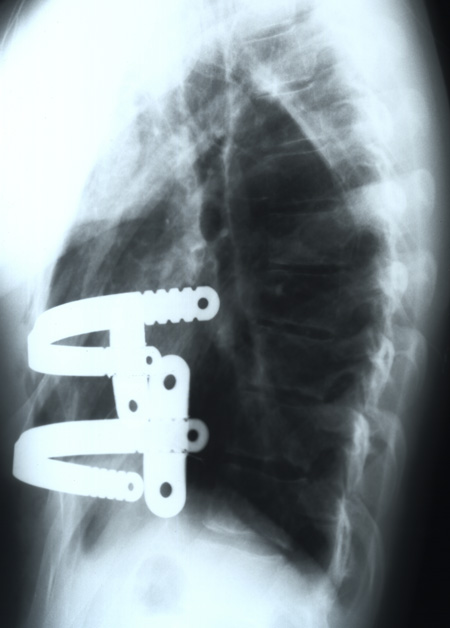
Ravitch open surgery – it consists of the resection of the deformed costal cartilage and sternotomy on demand in order to straighten the chest wall, which could be together with a metal splint fixation so that it gives stability to the chest wall and also reduces postoperatory pain. It is a long-term surgery entailing costal resections and osteotomies, blood loss and a visible scar. The current tendency is to indicate increasingly less this kind of surgery.
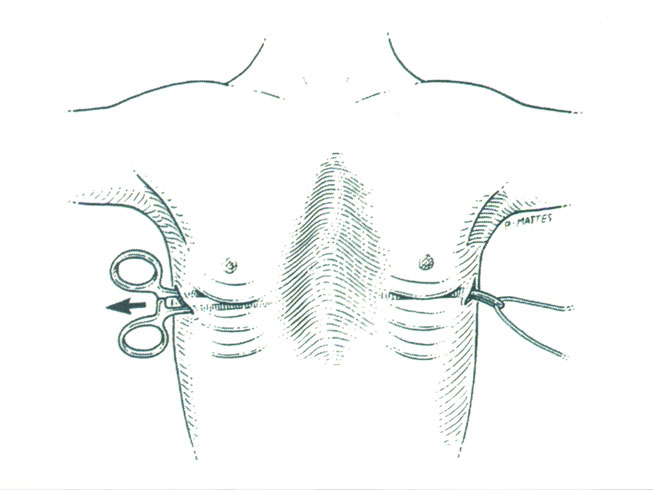
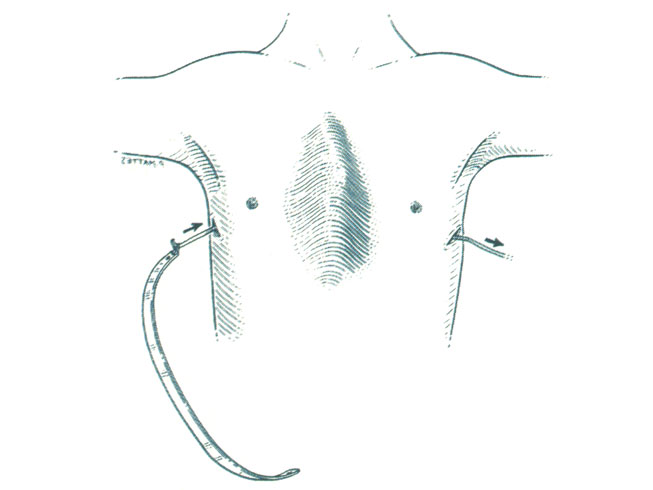
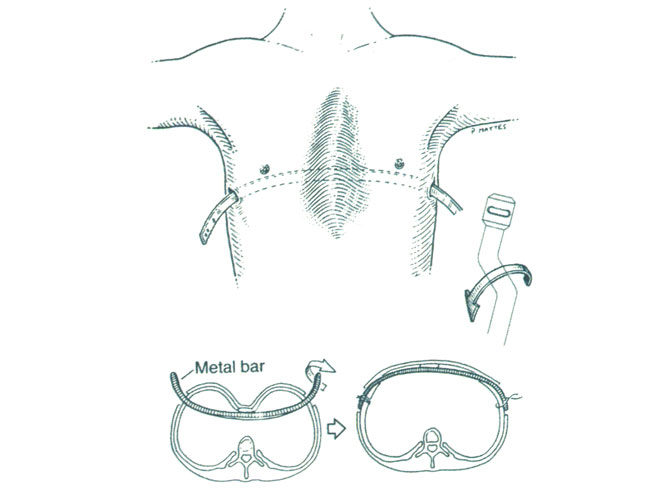
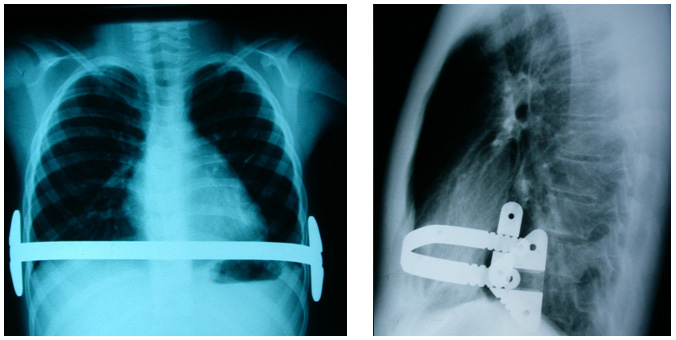
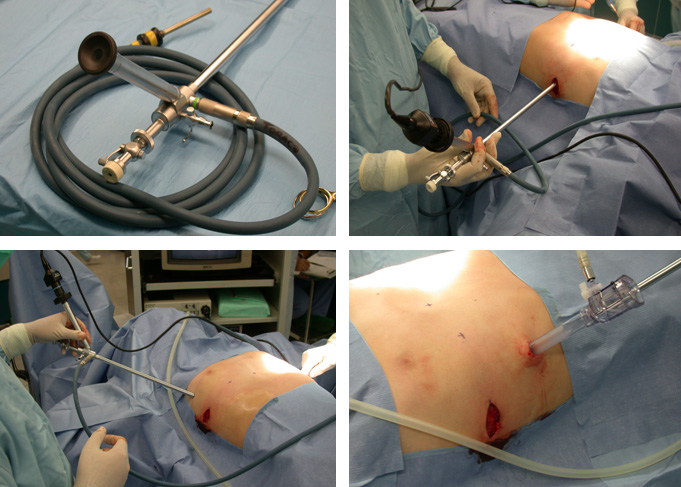
Another procedure is the Nuss minimally invasive technique, which consists of introducing the metal splint through a minor costal incision in the thorax under thoracoscopic vision. This bar is modelled suitable and lifts the sternum depression and the ribs when turning it. This is a highly well-accepted technique in the surgical community – it does not require any bone resection and only leaves two small scars in the thorax laterals. It requires a close monitoring of the postoperatory pain. Patients normally tolerate it suitably, since there are fewer important comlpications and it provokes a great satisfaction for the children and their relatives, and results are good, stable and conclusive. The bar must remain in situ for a minimum of two years before taking it out.
The existing therapeutic option is to fill up the pectus defect with different types of materials. Usually, it is used in mild cases and void of symptomatology.
One can resort to silicone prostheses which are either ideally suited, or made with materials like an injectable gel that are shaped throught digital compression to the defect. These are also recommended to correct little postoperatory consequences in order to match the shape of the chest wall, chiefly at the moment of the splint removal and if possible once the patient's growth has concluded.
Some of these materials present the inconvenience of having to be replaced as time goes by.













© Copyright 2009 pectusforum.com